Did you know that gum disease affects most people at some stage during their life?
Maintaining good gum and dental health is the key to preventing gum disease. Healthy gums are critical to a healthy mouth; allowing your teeth need to be embedded in firm, healthy gum tissue. Unhealthy gums can lead to major long term problems and costly treatments.
What is gum disease?
Periodontal (gum) disease is a serious illness usually caused by poor oral hygiene and the buildup of plaque and bacteria on the teeth. There are two stages of gum disease, Gingivitis and Periodontitis.
Gingivitis
The early stages of gum disease are called Gingivitis. Gingivitis usually occurs as a result of poor oral hygiene. As bacteria and plaque build up on the teeth, especially near the gums, they cause the gums to become red, inflamed and tend to bleed easily. Because gingivitis is a mild form of gum disease, it can usually be reversed with thorough brushing and flossing combined with regular visits to the dental hygienist and dentist. Fortunately there is usually no bone or tooth loss at this stage of gum disease.
Periodontitis
When gingivitis is left untreated it can develop into a more severe condition called periodontitis. Periodontitis occurs when the gums become inflamed and pull away from the teeth, forming gaps between the tooth and the gums. These are called periodontal pockets, Plaque and bacteria get trapped in these pockets which cause further inflammation, and in turn weakens the tooth, bone, and gums. Because the body’s immune system attempts to fight this bacteria by breaking it down, it can begin to attack the bone and gums that hold the teeth in place.
If left untreated, periodontitis can lead to bone and even tooth loss. Periodontitis has been linked to severe systemic diseases including diabetes, heart disease, and lung disease.
There are different types of periodontitis:
Agressive Periodontitis
This usually occurs patients who have no other health issues. Aggressive periodontitis is characterised by gums quickly detaching from teeth and rapid bone loss.
Chronic Periodontitis
The most common form of periodontitis, this is characterised by the formation of multiple periodontal pockets and severe inflammation and recession of the gums. The gums tend to detach from the teeth at a slow but steady rate. While most prevalent in adults, chronic periodontitis can occur at any age.
Periodontitis From Systemic Diseases
Sometimes periodontitis can result from more severe systemic illnesses such as diabetes, heart disease and lung disease. It generally occurs at a young age and progresses as the patient grows.
Necrotising Periodontal Disease
This form of periodontitis is an infection that affects the gingival (gum) tissues, periodontal ligaments and alveolar bone. It most commonly occurs in patients who suffer from systemic conditions such as malnutrition, immunosuppression and HIV infection.
Diagnosing Gum Disease
Your dentist or dental hygienist will diagnose periodontal disease during your regular dental check up with a periodontal examination. A periodontal examination is when a small probe is used to measure the space between the teeth and gums. Healthy gums will have a space of no more than three millimeters. If periodontal disease is present, these spaces will grow larger over time, and usually be accompanied by inflamed and bleeding gums, and in more severe cases, tooth mobility.

Symptoms of Gum Disease
Some signs and symptoms of gum disease include:
 Red, swollen gums
Red, swollen gums
 Bleeding gums when brushing
Bleeding gums when brushing
 Constant bad breath
Constant bad breath
 Sensitive teeth
Sensitive teeth
 Painful when eating
Painful when eating
 Receding gums
Receding gums
 New spaces forming between teeth
New spaces forming between teeth
If you experience any of these symptoms you should make an appointment with your dental hygienist or dentist. Contact Shore Dental for an appointment today.
Causes of gum disease

The main cause of gum disease is poor oral hygiene, which results in the buildup of bacteria and plaque in the mouth. Without regular brushing, flossing and checkups with your dental hygienist, you place yourself at risk of gum disease. There are also many more genetic and environmental factors that can contribute to the onset of gum disease:
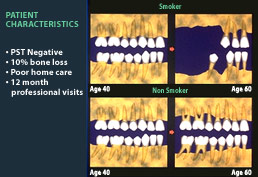
 Smoking
Smoking
 Stress
Stress
 Poor diet
Poor diet
 Grinding or clenching teeth
Grinding or clenching teeth
 Breathing through the mouth
Breathing through the mouth
 Conditions and medications that can suppress your immune system
Conditions and medications that can suppress your immune system
 Diabetes
Diabetes
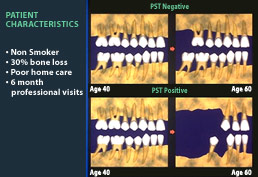
 Genetic predisposition and family history of gum disease
Genetic predisposition and family history of gum disease
 HIV and AIDS
HIV and AIDS
 Pregnancy
Pregnancy
 Birth control pills
Birth control pills
 Poorly fitting dentures
Poorly fitting dentures
 Genetics; males are more susceptible
Genetics; males are more susceptible
Can gum disease cause health problems beyond the mouth?

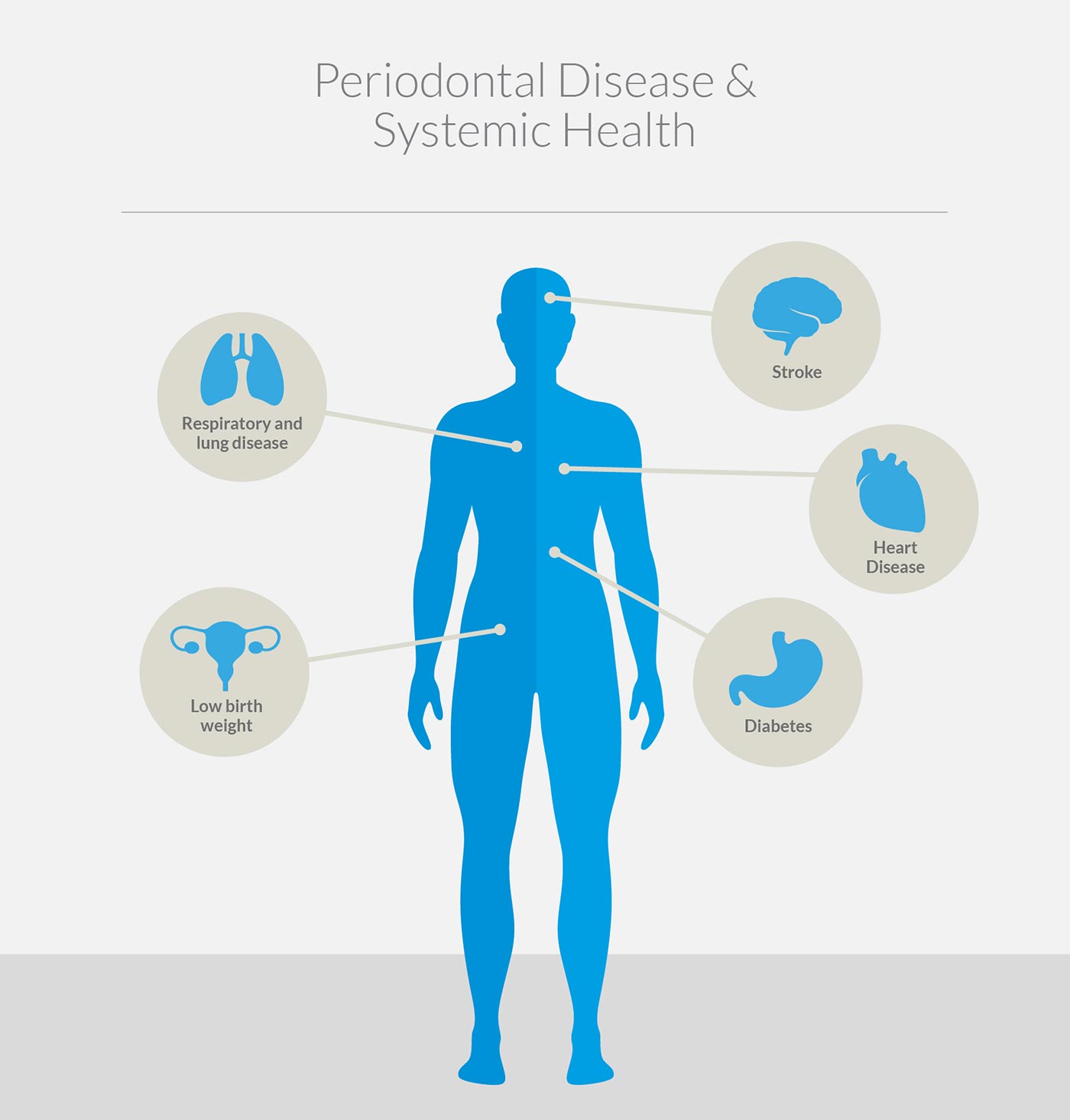
Periodontitis is closely linked to a number of systemic illnesses. Maintaining a healthy mouth not only means you will have good breath – it can also help to prevent more serious diseases. There are a number of ways oral bacteria can cause more severe ailments:
The buildup of bacteria in the mouth can enter the bloodstream, which can make its way to the heart
 Periodontal disease causes inflammation, which in turn elevates the white blood cell count in the body. This can affect a number of systemic illnesses
Periodontal disease causes inflammation, which in turn elevates the white blood cell count in the body. This can affect a number of systemic illnesses
 High levels of oral bacteria can weaken the immune system, which can lead to a number of more serious illnesses
High levels of oral bacteria can weaken the immune system, which can lead to a number of more serious illnesses
Serious systemic illnesses linked to gum disease include:
Heart disease
 Respiratory and lung disease
Diabetes
Respiratory and lung disease
Diabetes
 Stroke
Stroke
 Low birth weight
Low birth weight
To read more about how and why your dentist acts to diagnose and treat periodontal disease, look at the European Federation of Periodontology manifesto.
Preventative Dental Health

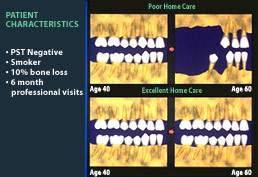
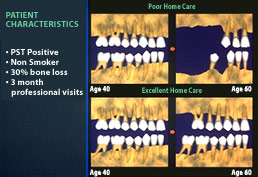
Gum disease is preventable. While gum disease affects most of us at some stage during our life, it is important to realise that it doesn’t have to. Careful regular teeth cleaning and visits to the dentist and dental hygienist are key to preventing gum disease and other serious oral health issues.
How to keep your teeth and gums healthy

The key to preventing oral health problems is proper dental hygiene. Your dental hygienist can show you the correct way to brush your teeth and gums, and how to floss properly to ensure you are removing as much plaque and bacteria as possible. Your dentist may also recommend using a vibrating electric toothbrush or miniature brush for cleaning in between your teeth.
To maintain good oral health you need to:
 Eat a healthy, balanced diet
Eat a healthy, balanced diet
 Limit sugary foods
Limit sugary foods
 Brush your teeth twice daily for two minutes
Brush your teeth twice daily for two minutes
 Visit the dentist every six months
Avoid smoking
Visit the dentist every six months
Avoid smoking
 Drink plenty of water
Drink plenty of water
To learn more about maintaining your oral health, please visit our Dental Hygiene page.
Treatment of gum disease
If you experience any signs or symptoms of gum disease, your dentist or dental hygienist should do a full periodontal examination to determine the severity of the condition. They should also ask you about your medical history, as some conditions may impact on your oral health or be exacerbated by it.
Depending on the severity of your condition, you may receive one of the following treatments:
Periodic scale and clean
If your gum disease is diagnosed in the early stages and no damage has been detected, your dental hygienist will recommend a periodic scale and clean. This removes disease-causing calculus, plaque and staining. Simply having your teeth professionally cleaned at least every six months will significantly slow down the progress of periodontal disease. If the disease has progressed, you may require deep scaling and root planing. This procedure removes plaque and calculus from the roots of the teeth and deep periodontal pockets, helping the gums to heal and the pockets to shrink in size. If the infection is causing you pain, your dentist or hygienist can recommend treatments such as a special mouth rinse, pain medication or a PerioChip, which is inserted into the periodontal pocket after treatment.
Your dental hygienist will also educate you on how to improve your dental hygiene. To learn more about this, visit our Dental Hygiene page.
What's the difference between hand scaling and ultrasonic scaling?
Periodontal scaling can be done either by hand or with an ultrasonic scaler. Hand scaling is done with a small instrument which effectively scrapes away built up plaque from your teeth. Ultrasonic scaling is done with an electronic device which removes plaque through small, rapid movements.
Gum surgery
In severe cases of periodontitis, deep scaling and root planing may not be sufficient to treat the disease. In these cases, surgery may be required to reduce the size of the periodontal pockets. Your dentist will refer you to a Periodontist who specialises in gum treatments.
There are two types of gum surgery to treat periodontitis:
Flap Surgery
In order to clean the very deep periodontal pockets, the periodontist will lift back the gums to access and clean the area properly. When all plaque, calculus and bacteria is cleaned away, the gum is replaced and stitched back into place, allowing them to heal properly.
Bone and Tissue Grafts
Bone and tissue grafts can be used in addition to flap surgery. Where gum and bone loss has occurred, grafts of natural or synthetic bone and tissue are used to replace the lost tissue. This promotes new bone growth, which helps to build healthier teeth and treat periodontitis in the long term.
Patient Case Studies
See examples of real Shore Dental patient case studies in our Smile Gallery